Introduction
The progression of global aging stands as one of the most significant social transformations of the 21st century, exerting profound effects on healthcare and long-term care systems, economies, and social security frameworks. According to United Nations estimates1, the global population ages 65 and up surpassed the number of children under age 5 for the first time in 2018. In 2022, the worldwide population of individuals ages 65 and up reached 771 million, approximately tripling the figure from 1980.
Projections indicate that this trend will continue, reaching 994 million by 2030 and 1.6 billion by 2050 (Figure 1). This acceleration in aging is not confined to high-income nations and is also occurring rapidly in low and middle-income countries, necessitating comprehensive responses in nutrition, healthcare, and welfare. Despite being a highly prevalent issue among older adults, malnutrition has frequently been underestimated, and implementation of appropriate screening and intervention strategies remains inadequate. Reports from the European Society for Clinical Nutrition and Metabolism (ESPEN)2 indicate that less than 10% of community-dwelling older adults and up to two-thirds of hospitalised older patients are malnourished or at risk of malnutrition. Malnutrition is not merely a deficiency in nutrients, but also a critical health concern directly linked to diminished physical function, impaired immunity, sarcopenia, increased susceptibility to infections, pressure ulcer development, and elevated mortality risk (Figure 2). The recently proposed concept of oral frailty suggests that age-related decline in oral function influences the progression of systemic frailty and sarcopenia.
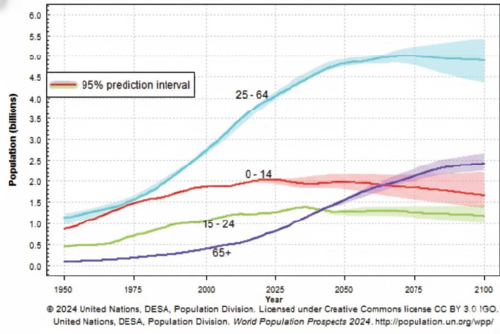
Figure 1. Trends and Projections of the World Population by Broad Age Groups
|
| Adapted from 2024 United Nations, DESA, Population Division. World Population Prospects 2024. This line graph illustrates the historical trends and future projections of the global population from 1950 to 2100, categorised into four broad age groups: 0-14; 15-24; 25-64, and 65 and up. The data indicate that around 2018, the global population ages 65 and up surpassed the population ages 0-14 for the first time. The graph further projects a continued increase in the elderly population and a decline in the younger population in the coming decades. |
|
Figure 2. Proposed algorithm for management of oropharyngeal dysphagia in the elderly
Adapted from Rofes, L., Arreola, V., Almirall, J., Cahn, M., Campins, L., Garcia-Peris, P., Speyer, R., & Clave, P. (2011). Gastroenterology research and practice, 818979, Figure 2, Copyright © Hindawi Publishing Corporation (2011 ). |
| In frail or elderly patients, oropharyngeal bacterial colonisation, impaired oropharyngeal clearance, and dysphagia can lead to decreased swallowing safety and efficiency, resulting in aspiration, malnutrition, and dehydration. If these conditions persist, they potentially can lead to sarcopenia, a weakened immune system, delayed wound healing, hypotension (affecting the kidneys, cardiovascular syste,m and consciousness), and ultimately, exacerbation of frailty, reduced functional capacity, pressure ulcers, opportunistic infections, and increased morbidity and mortality. |
Oral function and malnutrition in older adults
The decline in oral and swallowing function associated with aging is a significant contributor to malnutrition in older adults, representing a global public health challenge. A 2023 systematic review and meta-analysis3 reported a global malnutrition prevalence of 18.6% in older adults, with the highest rates in the African region (35.7%), followed by the Americas (20.3%). Furthermore, the prevalence of malnutrition (32.5%) and the risk of malnutrition (46.8%) are notably high among older adults with dementia4. Deterioration of oral and swallowing function with age, often termed oral frailty5, entails a complex interplay involving reduced muscle strength, decreased tongue pressure, impaired masticatory ability, and diminished salivary secretion, leading to decreased food intake and restricted dietary choices. This results in insufficient nutrient intake, contributing to reduced physical function, weakened immunity, and overall deterioration in health status. The prevalence of oral frailty in older adults has been reported at 32%6, underscoring the importance of its prevention and management. Therefore, maintaining oral and swallowing function is an indispensable element in preventing malnutrition and extending healthy lifespan in older adults, necessitating early assessment and a comprehensive support system involving multidisciplinary collaboration.
Assessment methods
Standardised screening tools have been developed for early detection of malnutrition in older adults, with the following tools in particular used widely.
Nutritional status assessment
Mini Nutritional Assessment (MNA)
The MNA is a tool developed for rapid and comprehensive assessment of nutritional risk in older adults. It is simple and quick to administer, non-invasive, and provides a holistic evaluation of nutritional status7. It comprises 18 items across four components: anthropometric assessment (weight, height, weight loss); general assessment (lifestyle, medication, mobility); dietary assessment (number of meals, food and fluid intake, independence in feeding); and self-assessment (self-perception of health and nutrition). Individuals are categorised into one of three groups: normal nutritional status, at risk of malnutrition, or malnourished.
Global Leadership Initiative on Malnutrition (GLIM)
Criteria: In 2019, major global nutrition societies - including ESPEN, ASPEN, PENSA, and JSPEN - collaborated to establish the Global Leadership Initiative on Malnutrition (GLIM) criteria8. These criteria provide a unified diagnostic framework for malnutrition, requiring the fulfilment of criteria from two categories. In older adults, implementation of GLIM criteria is considered to improve diagnostic accuracy and the timing of interventions (Figure 3).
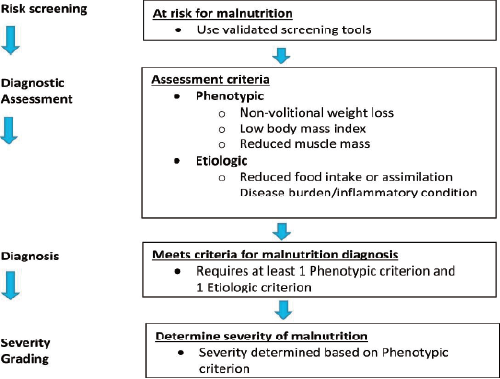
Figure 3. GLIM diagnostic scheme for screening, assessment, diagnosis, and grading of malnutrition.
|
|
From Cederholm T. et al. (2019). GLIM criteria for the diagnosis of malnutrition - A consensus report from the global clinical nutrition community. Clinical Nutrition, 38(1-9). https://doi.org/10.1016/j.clnu.2018.08.002 This illustrates the diagnostic process for malnutrition based on the GLIM criteria. A positive result in risk screening leads to the evaluation of phenotypic (weight loss, low BMI, reduced muscle mass) and etiologic (reduced food intake, malabsorption, disease burden/inflammation) factors. A diagnosis of malnutrition is made if at least one criterion from each category is met. |
Swallowing function screening
Modified Water Swallowing Test (MWST)
The MWST is a safe and early method developed to screen swallowing function in acute patients and those suspected of severe dysphagia9. It involves having the patient swallow a small amount of water (3 ml) at once, while observing for signs of choking, coughing, or wet vocal quality.
Eating Assessment Tool (EAT-10)
The EAT-10 is a self-administered questionnaire that scores 10 items related to subjective symptoms of swallowing difficulties. It assesses the extent to which patients experience problems with eating and swallowing, and their severity. A score of 3 or higher indicates a high probability of dysphagia10. In addition to screening for potential swallowing disorders, it can also be used to evaluate the effectiveness of interventions, such as swallowing training, over time.
Prevention and intervention strategies
Comprehensive interventions are essential for preventing and improving the decline in oral and swallowing function in older adults. First, regular oral care is known to reduce the risk of aspiration pneumonia11, and dental visits, denture management, and thorough oral hygiene are recommended. Swallowing rehabilitation aims to improve swallowing function using strengthening exercises for swallowing muscles and compensatory swallowing techniques. In particular, adjusting food texture is crucial.
The International Dysphagia Diet Standardisation Initiative (IDDSI) provides a globally consistent classification and stepwise modification of solid foods and liquids, promoting appropriate dietary management for individuals with dysphagia12. Adjusting to appropriate food textures reduces the risk of aspiration and enables safe and efficient eating. Specifically, thickening liquids play a vital role in controlling flow rate and ensuring safe pharyngeal transit. The concentration of thickening agents should be adjusted appropriately based on individual swallowing function, and caution should be exercised, as excessive thickening can increase the risk of aspiration and reduce intake motivation. Furthermore, use of oral nutritional supplements (ONS) is effective in reducing the risk of malnutrition (Figure 4)13. Supporting these efforts requires collaboration among a multidisciplinary team, including physicians, dentists, speech-language pathologists, registered dietitians, and nurses. Furthermore, social support measures, such as communal dining and meal assistance programmes, are important strategies to prevent social isolation.
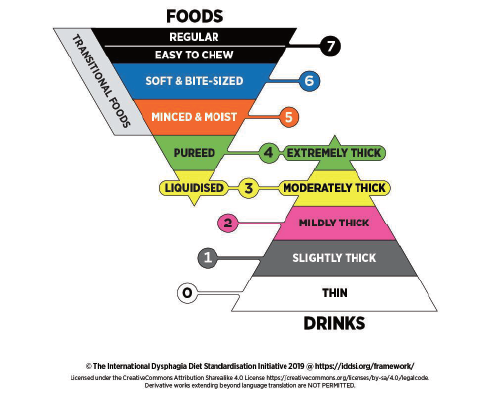
Figure 4. The IDDSI Framework (the Standard)
|
|
Adapted from © The International Dysphagia Diet Standardisation Initiative 2019 @ https://iddsi.org/. Licensed under the Creative Commons Attribution Sharealike 4.0 License https://creativecommons.org/licenses/by-sa/4.0/legalcode. Derivative works extending beyond language translation are NOT PERMITTED. The IDDSI framework comprises a continuum of eight levels (0-7), in which drinks are measured from Levels 0-4, while foods are measured from Levels 3-7. The IDDSI framework provides a common terminology to describe food textures and drink thickness. |
Optimisation of food texture
Older adults with dysphagia often require more time and effort for eating compared with those consuming a regular diet, consequently increasing the risk of reduced food intake. Texture-modified diets (TMDs) are dietary interventions that alter food hardness, adhesiveness, cohesiveness, and particle size to mitigate the risks of aspiration and choking. However, inappropriate selection of food texture has been reported to not only decrease safety, but also lead to insufficient nutrient intake, thereby increasing the risk of malnutrition14. In particular, choosing foods that are too hard for adequate chewing and swallowing, or conversely, excessively soft foods with low nutrient density, can result in decreased intake of energy and macronutrients. Furthermore, alterations in food texture have been reported to decrease mealtime satisfaction15. Meals are not merely a means of nutritional sustenance, but also impact quality of life (QOL) significantly. Diminished mealtime satisfaction can decrease patients' motivation, potentially initiating a negative cycle of further reduced food intake. Therefore, in addition to selecting an appropriate food texture tailored to the patient's swallowing function, it is crucial to consider nutritional aspects and devise strategies that preserve the enjoyment of eating as much as possible.
Future perspectives and challenges
Addressing malnutrition and impaired swallowing function in older adults necessitates the introduction of new technologies and social systems. In recent years, the use of artificial intelligence (AI) for swallowing function screening and remote swallowing rehabilitation (telerehabilitation) has attracted attention, with the potential to expand support for home-dwelling older adults. Furthermore, the World Health Organisation's Integrated Care for Older People (!COPE) guidelines advocate for integration of nutritional, oral, and swallowing management into community-based integrated care systems16. Particularly in low-resource settings, widespread adoption of simple and low-cost assessment tools and development of support systems involving community residents are needed urgently. Moreover, development of intervention strategies that are sensitive to multicultural contexts is indispensable, requiring the provision of individualised nutritional support while respecting diverse food cultures and values. Construction of new models for nutritional management in older adults, thereby integrating scientific evidence with digital technologies and social collaboration, is essential.
Conclusion
As the global population continues to age, malnutrition and related health issues in older adults are becoming increasingly significant public health challenges. Addressing these problems requires more than simply improving nutritional intake; it necessitates integration of comprehensive assessment and intervention to integrate oral and swallowing function into healthcare and long-term care systems. Maintaining oral and swallowing function is not merely about survival, but is the 'key' to enabling older adults to maintain their dignity, live independently, and enhance their quality of life.
-
Publication Date:November 26, 2025
-
Category:Nutrition
HosCom International 2025 Vol. 2
